The importance of visualization in laparoscopic surgery
The ability to look within a patient’s body cavity was a long-held desire in medicine.
Until the early 19th century, the ability to diagnose and treat a patient’s condition, unless clearly visible or easily palpated, was a secret the body would hold onto until either surgery, or an autopsy were performed.
Early exploration into laparoscopic surgery
In 1865, Sir Francis Richard Cruise of Dublin was the first to explore a body cavity, the empyema cavity in the thorax of an 11-year-old girl. Later Georg Kelling (1866-1945) in Germany was the first to examine the abdomen with an endoscope, a procedure that he called “celioscopy.” He found that insufflation of the abdomen with air, a procedure that he had tried in an unsuccessful attempt at controlling gastrointestinal haemorrhage, was a good way to create working space within the abdominal cavity.
Despite the work of Cruise and Kelling, Hans Christian Jacobaeus (1879-1937) has been called “the inventor of human laparoscopy and thoracoscopy.” [i] He performed diagnostic laparoscopy on 17 patients with ascites, an experience which he published in 1910, in Sweden.
Pneumoperitoneum was a necessary precedent to the development of laparoscopy. It was originally a radiological procedure to outline the viscera on plain films and fluoroscopy. Arthur Stein, a gynaecologist, and William Stewart, a radiologist, introduced the modality in New York, America in 1919. They used an anaesthesia bag to inflate the free abdominal cavity with air or oxygen through a standard spinal needle. Two years later, Walter Alvarez, an internist in San Francisco, reported the use of carbon dioxide for the procedure. The peritoneal cavity absorbed carbon dioxide within a few minutes, a distinct advantage over oxygen or air, which sometimes remained in the abdomen over days, causing prolonged discomfort. [ii]
Gynaecologists are credited as the first specialists to fully devote themselves to laparoscopy and its therapeutic potential. Raoul Palmer, a gynaecologist at the Hospital Broca in Paris, and his wife Elizabeth started to perform laparoscopic procedures in occupied Paris in 1943. As the war ended everything became scarce, from household items to hospital supplies. Raoul recognised the importance of controlling the amount of pressure within the abdomen, so he added a manometer to his insufflator, which he assembled from parts he found in storage areas in his hospital. Unable to drive to nearby towns because of gasoline rationing, he rode his bicycle to scrounge the carbonic acid necessary to generate carbon dioxide gas. [iii]
The next major advancement was to be nearly forty years later, when in 1980 the first appendix was removed laparoscopically by Dr Kurt Semm, in Kiel, Germany. Later that decade in 1985 Erich Muhe, a general surgeon in Boblingen, Germany, and in 1987, Phillipe Mouret, a gynaecologist in Lyon, did the first laparoscopic cholecystectomies. [iv,v]
The future of laparoscopic surgery had to expand beyond the small number of gynaecologists with a special interest in laparoscopy and into general surgical practices. Mouret did his two-and-a-half-hour cholecystectomy on his side lying on the patient’s right thigh to keep his eye over the objective of the scope. “[It] had been a contortionist’s exploit,” he said. For laparoscopic surgery to be adopted, it simply had to be made easier to perform. [v]
Technological advancements in laparoscopic surgery
Fiber optics made two fundamental technological contributions to medicine: flexible endoscopy and proximal illumination of the abdominal cavity. The former revolutionised the practice of gastroenterology; the latter provided the light needed for laparoscopic surgery.
Solid state camera technology of the 1980s, created the first wave of electronic digital cameras and portable video systems [vi], at that time believed to be the final piece of the puzzle. As video monitors improved the images on high-definition displays, surgeons had the optical resolution they needed to discern the anatomical details necessary to perform surgical operations of increasing complexity. Their eye no longer locked onto the objective of the laparoscope held by one hand, surgeons could stand, view the operation on a video display, and perform standard operations using both hands.
Electrosurgery causes a new visualization issue
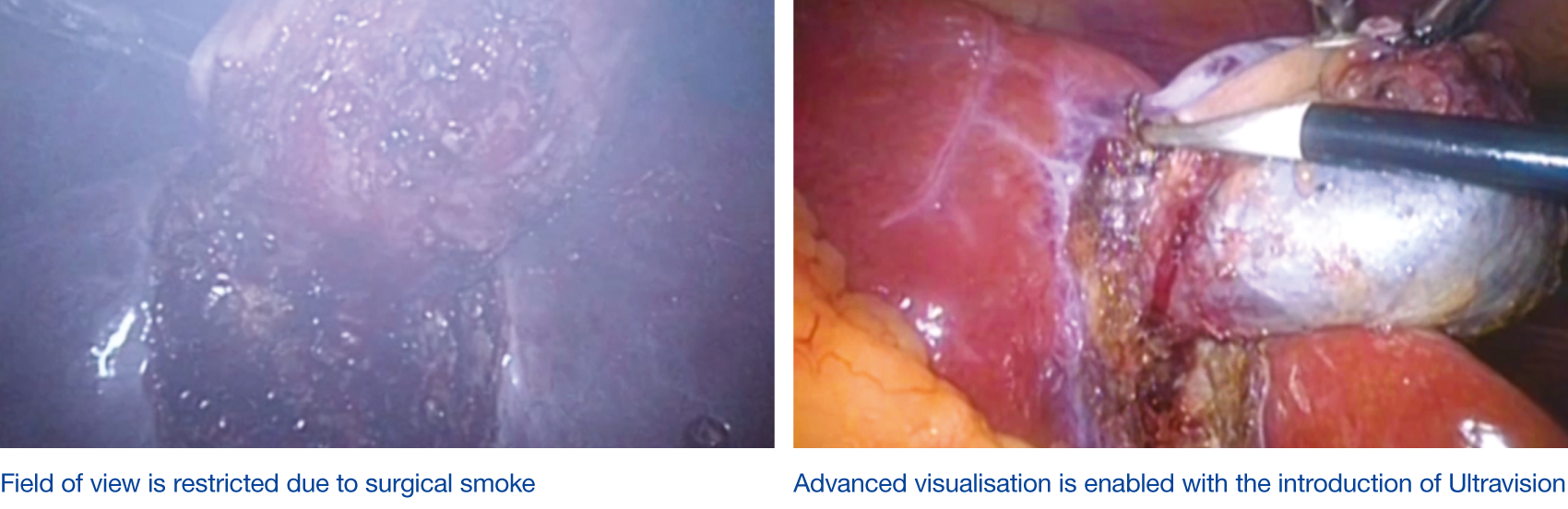
Despite the advances in picture quality, with new systems sporting 3D and/ or 4K pictures, another issue arose blemishing the coveted crystal-clear images – ‘smoke’, caused using electrosurgery devices. Smoke would now obscure the vision for the surgeon, slowing down the procedure or even resulting in errors. Original solutions to remove the smoke also affected pneumoperitoneum causing longer surgery times and increased patient exposure to CO2.
There are many devices now on the market to try and manage the issue of smoke in the peritoneal cavity, but few are as efficient as the Ultravision system. It can achieve smoke clearance to 99.9% within one minute of activation[vii]. It’s unique mode of action supresses smoke particulates, at the point of creation, enabling visual field clarity and providing the proper final piece of the jigsaw.
[i] Hatzinger M, Kwon ST, Langbein S, et al. Hans Christian Jacobaeus: Inventor of human laparoscopy and thoracoscopy. J Endourol. 2006 Nov;20(11):848-850.
(https://pubmed.ncbi.nlm.nih.gov/17144849/)
[ii] Alvarez WC. Use of CO2 in pneumoperitoneum. Am J Roentenol. 1921 Feb;8(2):71-72.
[iii] Litynski G. Raoul Palmer, World War II, and transabdomial coelioscopy. Laparoscopy extends into gynecology. JSLS. 1997; 1:289-292.
(https://pubmed.ncbi.nlm.nih.gov/9876691/)
[iv] Litynski GS. Endoscopic surgery: The history, the pioneers. World J Surg. 1999;23(8):745-753.
(https://pubmed.ncbi.nlm.nih.gov/10415199/)
[v] Mouret P. How I developed laparoscopic cholecystectomy. Ann Acad Med Singapore. 1996;25(5):744-747.
(https://pubmed.ncbi.nlm.nih.gov/8924020/)
[vi] Fossum ER. Camera-on-a chip: Technology transfer from Saturn to your cell phone. Technology Innovation. 2013; 15(3):197-209.
(http://ericfossum.com/Publications/Papers/2013%20NAI%20Tech%20Transfer%20from%20Saturn%20to%20Cell%20Phone.pdf)
[vii] Alesi Surgical report DREP-002, held on file.